Policy must address the disproportionate access to medical care on tribal nations, which could be a contributing factor to the increased COVID-19 mortality and infection rates among indigenous populations.
The coronavirus pandemic is the latest deadly infectious disease to disproportionately kill and infect indigenous people in the United States. In New Mexico, indigenous people make up roughly ten percent of the population but more than 50 percent of the COVID-19 infections during the initial spring 2020 wave. Infection rates of over 40 percent were experienced by the Mississippi Band of Choctaw Indians (MBCI). Both the Navajo Nation and MBCI at one point saw higher infection rates than anywhere else in the country, including New York City.

As was the case with previous deadly infectious diseases-which also disproportionately killed and infected indigenous people at higher rates than non-indigenous people- one should not look past the economic and social policies that contribute to this current and historical reality. Of the many factors behind these infection rates, I am choosing to focus on medical care accessibility by exploring immediate and long-term policy solutions which can increase access to adequate health care services in indigenous communities.
Federal Support Structures Currently in Place for Tribal Nations. Federal support of coronaviruses mitigation in tribal communities and for NA/AI populations includes a mixture of direct financial support to tribal governments and the establishment of federal grants for which tribal nations and organizations can apply. Despite multiple federal dollar sources, the slow pace in which tribal governments receive funds coupled with limited access to personal protective equipment, testing, and medical personnel prevents current supports from holistically supporting tribal communities. Federal-level policy grounded in the expressed needs of NA/AI communities is needed to equitable support tribal nations as they work to meet the medical needs of their communities epitomized by COVID-19 pandemic.
Learning from Pandemic Responses Across Tribal Nations. In recent months, many indigenous communities slowed the spread of coronavirus by exercising their tribal sovereignty to enforce curfews, mandate stay at home orders, create call centers, manage online databases, and staff incident command systems to provide support to tribal citizens. An example of this is the Navajo Nation, which as of September had conducted more than 100 thousand tests, placing this testing per capita rate among the highest in the United States.

So what now what. With an increased focus on the inequitable access to medical care during a global pandemic, what can federal and state level policy makers do to address to ongoing challenges of the coronavirus?
· Learn from the successes of indigenous communities globally and locally.
· Listen to and act on tribal leaders’ concerns.
· Examine federal funding structures through a lens of equity.
· Build on existing structures to support the medical infrastructure moving forward.
Oximeter Pulse Monitors. Indigenous communities in both New Zealand and rural Arizona found success with implementing oximeter tracing systems to monitor health from home and act as a contact tracing system. In tribal communities across the United States, hospitals are rapidly approaching full capacity. By funding technology that empowers individuals to monitor non-urgent cases from home, hospital space and medical personnel will have greater capacity to serve those with the highest need. In order to implement this system, funding would be needed to support both the $15 oximeter pulse monitors and the hiring of staff to help with training and distribution. It is important to acknowledge that this structure will not solve the very real challenge of inequitable disease spread or death and instead seeks to provide a remedy for overwhelmed hospitals.
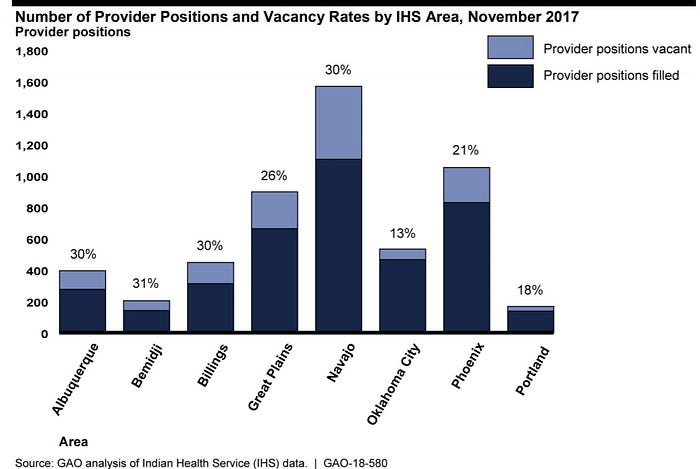
Expanding Indian Health Services (I.H.S.) Doctor Cultivation Program. Currently, I.H.S. offers $20 thousand in federal student loan forgiveness to increase the number of physicians serving rural I.H.S. facilities. According to the Government Accountability Office, the largest tribal nation in New Mexico, the Navajo Nation, consistently maintains a physician vacancy of 30 percent. With the overwhelming need for medical care during the coronavirus pandemic, it is essential that this vacancy rate is addressed. Extending the program’s benefits to four years will double to cost to total of $20.8 million over four years. Extending the length of the program fosters a huge opportunity to leverage physician’s expertise to support high school medical pathway programs. A goal that we should always consider when creating policy is how to support communities to lead the way, by partnering with local schools, doctors from this program can guide students who are interested in becoming a doctor and follow them throughout their high school careers. This is a similar approach to the Educator’s Rising program that already exists throughout the county.
I recommend implementing a combination of Oximeter Contact Tracing and expanding I.H.S.’s loan repayment program. These two policies present both an immediate and long-term opportunity to address access to medical care and are responsive to the additional support communities are explicitly requesting.
